We use cookies on this site to improve our service, perform analytics, and remember website preferences. By using this site, you consent to these cookies. For more information visit our Privacy Policy
Mapping complexity for safer patient transfers
HHF collaborated with the UHN Transfer of Accountability and Information Steering Committee to improve patient safety during patient transfers from the emergency department to inpatient units. Through ethnographic research and process mapping, HHF identified success measures and opportunities to standardize communication and accountability during high-risk transitions in care.
In collaboration with
UHN Transfer of Accountability and Information Steering Committee
Services
Clinical Observations, Ethnographic Research, Contextual Interviews, Process Mapping, Recommendations Report
Challenge
Transitions in care are one of the top contributors to serious safety events in hospitals. For example, when a patient moves from the emergency department to inpatient care, accountability and information are transferred simultaneously. Without clear processes and shared expectations, variability during these handoffs can increase risks of errors that may affect patient safety.
The University Health Network (UHN) is aiming to standardize its Transfer of Accountability and Information practices (TOA/I) across sites. TOA/I refers to the timely and accurate communication of relevant information when responsibility for a patient’s care permanently shifts from one team to another. In high-volume, high-pressure environments like the Emergency Department (ED), these permanent transfers to inpatient units are especially complex and sensitive.
While policies define how TOA/I should occur, there is limited visibility into how ED-to-inpatient unit transfers unfold in practice. To address this challenge, the TOA/I committee engaged HHF to conduct observational research and develop process maps to understand how patient transfers work in practice, successful elements that can be standardized in other areas where TOA/I occurs, and barriers that can be removed for quick and effective transfers.
We examined ED-to-inpatient unit transfers through direct observation and staff engagement, with two objectives: clarify the current-state workflow, and identify system-level factors that influence safety and impact staff and patient experience.
Process
Discovery
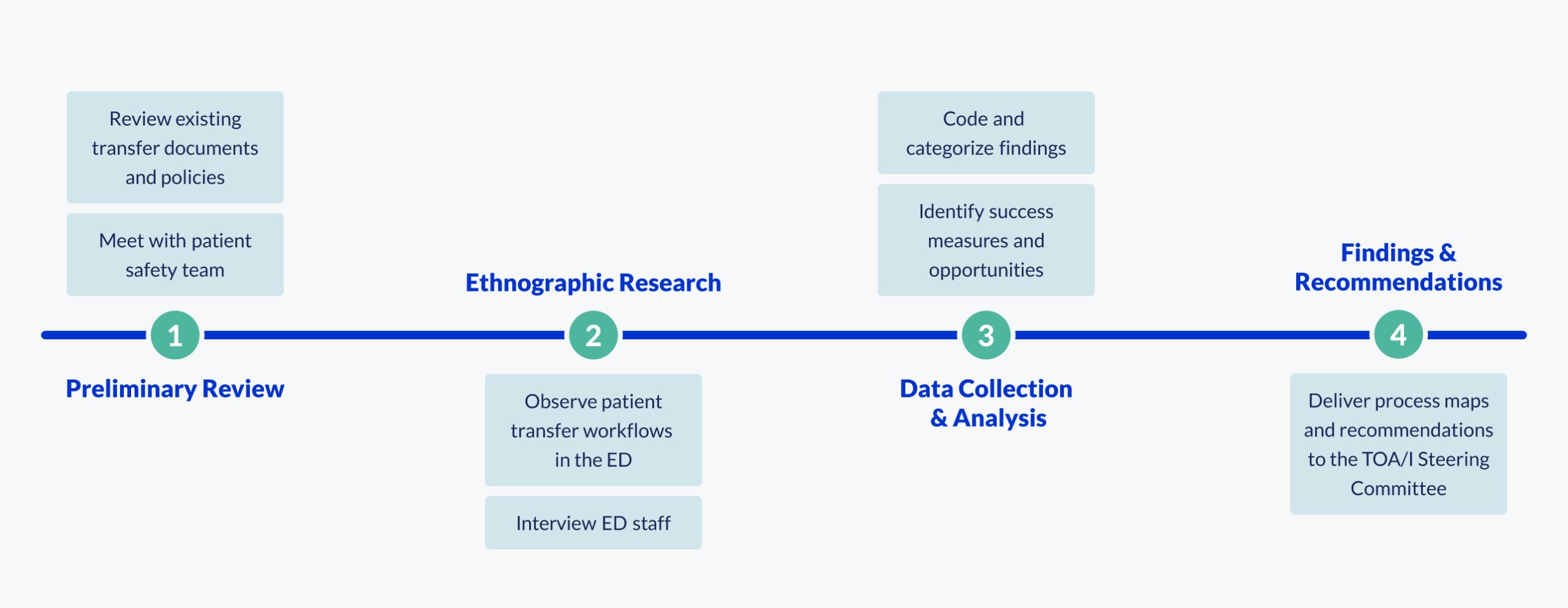
We began by meeting with the TOA/I patient safety team to understand the current standards, processes, and expectations for transfers out of the ED. This informed our focus on three key areas during fieldwork: technology, teamwork, and the clinical environment.
Over one week we conducted ethnographic research by observing permanent transfers in which a patient’s care and accountability moved from the ED to an inpatient unit and interviewing 14 staff members in the ED. This allowed us to examine how communication patterns, technology, environmental pressures and departmental coordination shape the transfer process in practice.
Analysis and Synthesis
While observations were ongoing, our designers collaborated with our human factors specialists to develop process maps that visualized the full ED-to-inpatient transfer journey. We immersed ourselves in existing UHN documentation about inpatient unit flow and transfer policies, and interviewed the TOA/I steering committee to better understand the organization’s expectations and processes around patient transfers.
We synthesized the data into five themes related to external factors that influence the ED ecosystem: the technology used to track patients and initiate transfers (EPIC), hospital policies, inter-departmental and staff collaboration, and workflow variability. For each theme, we identified where processes and practices supported safe transfers and where variability introduced risk.
Overall, we identified:
- • 15 success measures that support safe patient transfers
- • 22 opportunities for improvement
We need efficient transfers out of the ED because you need to see the patients in the waiting room. The priority is seeing people as efficiently as possible before something bad happens while they are waiting to be seen.
ED Nurse

Design
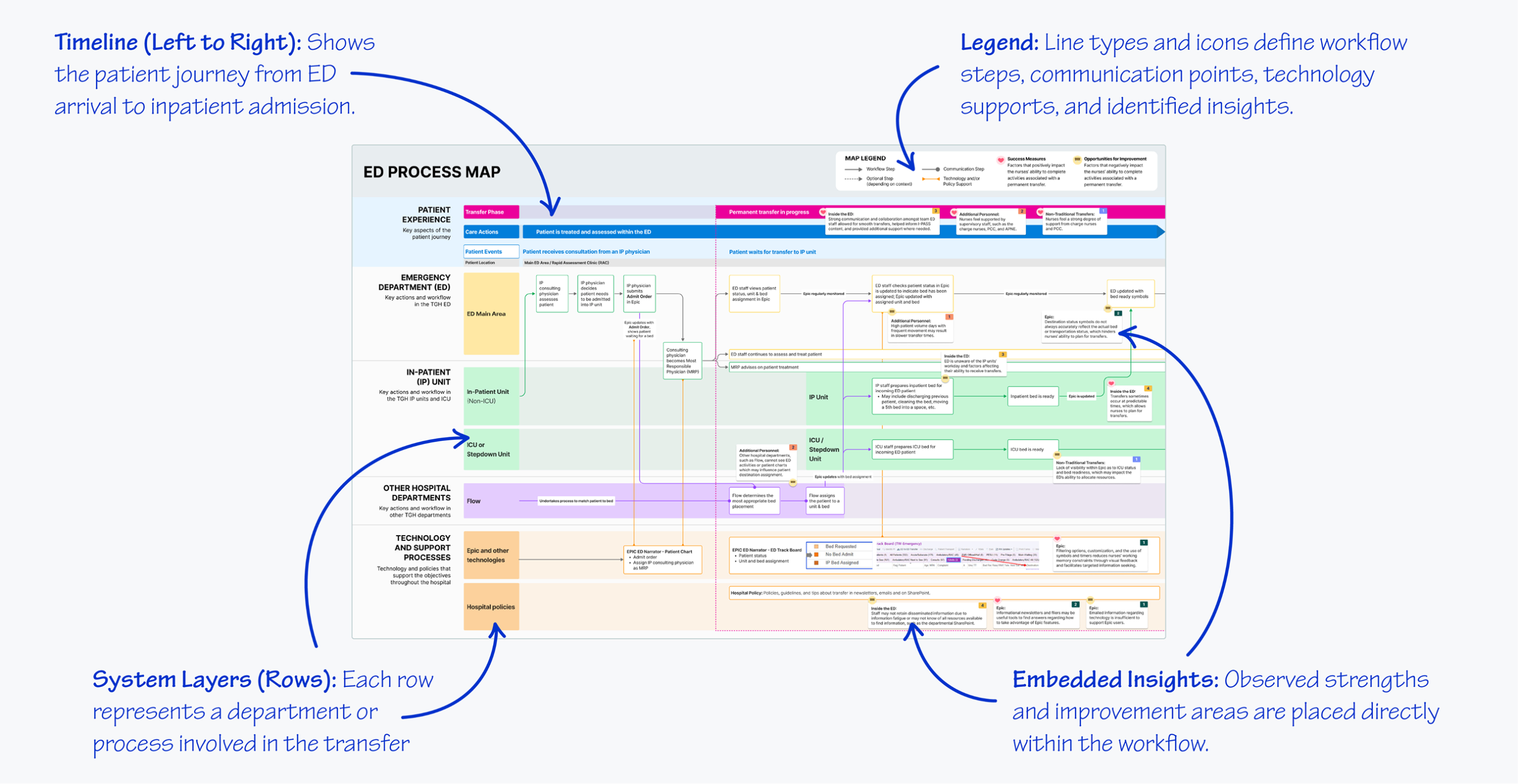
To translate our findings visually, our team developed detailed process maps to visualize the full ED-to-inpatient transfer journey. Each finding was mapped to specific steps in the transfer process, highlighting deviations from intended workflows and identifying targeted recommendations to improve patient safety.
Our maps displayed:
- Patient experience
- ED workflows
- Inpatient unit workflows
- Other hospital departments involved or closely linked within the TOA/I process
- Technologies and policies shaping decisions
These parallel workflow lanes revealed interdependencies that aren’t transparent to individual teams. We first mapped the current state, highlighting successful elements that must remain part of of the TOA/I process. We then overlaid safety risks, critical points, and opportunities for intervention to support decision making.
Outcomes
We provided the TOA/I committee and other stakeholders across UHN with findings, process maps, and recommendations that serve as actionable tools to guide decisions, plan next steps, and strengthen the transfer process.
These deliverables will support the TOA/I steering committee to:
- Standardize required transfer information
- Align sender and receiver workflows
- Define clear ownership of transfer activities
- Reduce reliance on informal workarounds
- Strengthen communication to patients during transfers
Permanent transfers are not simple handoffs. They are complex events. Making them safer requires shared visibility, aligned expectations, and coordinated workflows. This evidence-based approach will help the UHN TOA/I steering committeedesign safer, more reliable transfer processes moving forward.